This guide covers what FDA inspection readiness means in 2026, how to prepare before, during, and after an inspection, and a practical checklist for medical device, biotech, diagnostic, and pharmaceutical companies navigating an evolving regulatory landscape shaped by the new QMSR framework.
Key Takeaways
- Inspection readiness is a daily operating state, not a pre-visit sprint
- Documentation should tell a self-explanatory story — auditors cannot rely on verbal clarification to fill gaps
- Personnel must articulate the scientific rationale behind decisions, not just procedures
- A robust CAPA system demonstrates control better than zero findings
- Medical device manufacturers must meet QMSR transition requirements — the rule became effective February 2, 2026
What Is FDA Inspection Readiness — And What's New in 2026
FDA inspection readiness is the continuous organizational state in which documentation, personnel, processes, and facilities are maintained to withstand unannounced FDA scrutiny at any time. It's not a sprint triggered by advance notice — it's an always-on posture.
The 2026 Game-Changer: QMSR Takes Effect
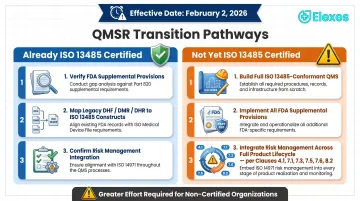
On February 2, 2026, the FDA's Quality Management System Regulation (QMSR) became effective, changing how medical device manufacturers demonstrate compliance. The rule amends 21 CFR Part 820 to incorporate ISO 13485:2016 by reference, creating alignment between FDA requirements and the international quality standard.
What this means in practice:
For companies already ISO 13485:2016 certified, the alignment reduces duplicative documentation requirements. Significant work remains, though. You must verify that FDA supplemental provisions are fully implemented:
- Complaint records (21 CFR 820.35)
- Labeling and packaging controls (21 CFR 820.45)
- Medical Device Reporting interfaces (21 CFR 803)
- Corrections and Removals (21 CFR 806)
- UDI requirements (21 CFR 830)
The historical terminology of Design History Files (DHF), Device Master Records (DMR), and Device History Records (DHR) now maps to ISO 13485 constructs. Inspectors will evaluate your Medical Device File and record control systems, not look for documents labeled "DHF."
Without ISO 13485 certification, the transition is more substantial. You need a complete ISO 13485-conformant QMS plus all FDA supplemental provisions. Risk management must be explicitly integrated across your product lifecycle — ISO 13485 clauses 4.1, 7.1, 7.3, 7.5, 7.6, and 8.2 all apply. Design and development controls per Clause 7.3 now clearly extend to some Class I devices and IDE devices as well.
Current Inspection Environment
FDA continues working through post-pandemic inspection backlogs while emphasizing a risk-based approach to scheduling. The agency's March 2026 FDARA Section 902 Annual Report documents substantial inspection activity supporting drug and device applications, though the FDA does not maintain a fixed inspection schedule for all facility types.
Two inspection priorities dominate 2026: data integrity across electronic records and audit trails, and assessment of companies' QMSR transition readiness. Device inspections now follow Compliance Program 7382.850, replacing the legacy QSIT inspection methodology.
Types of FDA Inspections: A Quick Overview
Pre-Approval Inspections (PAI): Triggered by marketing applications (NDA, ANDA, BLA, PMA, 510(k)) to verify manufacturing capability and data integrity supporting your submission.
Surveillance Inspections: Routine GMP assessments evaluating ongoing compliance at established facilities. Conducted under FDA's risk-based site selection model, these replace the historical fixed-interval schedule.
For-Cause Inspections: Unannounced visits triggered by adverse event reports, complaint patterns, or whistleblower referrals. These are the highest-stakes scenario — generally unannounced to protect evidence integrity.
BIMO Inspections: Focused on clinical investigator sites and sponsors to verify reliability and integrity of data supporting applications.
For-cause inspections test your real-time readiness when there is no time to prepare. The sections that follow walk through exactly what that readiness infrastructure looks like in practice.
Pre-Inspection Preparation: How to Build a Foundation for Success
Build a Cross-Functional Inspection Readiness Team
Effective preparation requires standing organizational infrastructure, not ad-hoc response:
- Appoint a dedicated project manager with QMS expertise and authority to mobilize resources across departments
- Identify subject matter experts (SMEs) from manufacturing, quality, regulatory, engineering, and post-market surveillance
- Document backup personnel for every key position — inspections don't wait for vacations or sick days
- Create a written rapid-response protocol detailing who gets notified, how the war room activates, and escalation procedures for unannounced inspections
Documentation: Build a Story, Not Just a Filing System
Inspectors assess whether your documentation tells a coherent, self-explanatory story of your quality system. Three requirements stand out:
- Naming and numbering conventions that show relationships between batch records, SOPs, specifications, and CAPAs — an investigator should be able to trace from a complaint to the related CAPA to the affected procedures to training records without asking questions
- Document biographies that track when and why significant changes occurred; version histories must capture rationale, not just dates
- Zero overdue reviews across all controlled documents — this is one of the clearest indicators of organizational control an investigator can see at a glance
Any document pulled at random should be self-explanatory. Context that requires verbal explanation is a documentation gap, not a communication strategy.
Train Personnel on Inspection Conduct, Not Just Procedures
General staff training covers:
- Answer only what is asked; do not volunteer information
- Clarify questions before answering
- Never speculate or guess
- Direct technical questions to appropriate SMEs
SME preparation requires depth:
Role-specific training must go beyond SOP recitation. Present SMEs with realistic scenarios — an out-of-specification result traced to environmental contamination, a discrepancy between batch records and equipment logs, an equipment failure during a critical manufacturing step.
The goal is articulating not just what was done, but the scientific rationale behind each decision.
Develop role-specific skill matrices documenting demonstrated proficiency, not just training attendance. An inspector wants to see that your validation engineer understands validation principles, not that they attended an 8-hour class.
Facility and Physical Readiness
Designate a workspace for the investigator containing no confidential records. Equip it with a table, chairs, power outlets, and Wi-Fi access.
Prepare a war room — a separate space for your inspection support team to coordinate responses, review documents before release, and anticipate next requests.
Maintain GMP-standard cleanliness across all production areas, utilities, and equipment. Maintenance histories, calibration records, and equipment logbooks must be immediately accessible.
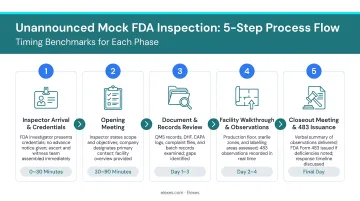
Conduct Mock Inspections Without Notice
Mock inspections reveal gaps that internal reviews routinely miss:
- Conduct without advance notice to test true readiness, not rehearsed performance
- Use experienced external auditors familiar with current FDA expectations and QMSR requirements
- Test document retrieval speed — two-minute standard for any requested record
- Practice SME interviews under pressure, including unexpected technical questions
- Time all responses and identify bottlenecks in your process
Elexes conducts QMS readiness assessments and mock audits across medical device and diagnostic categories, drawing on 50+ years of collective regulatory experience to identify documentation gaps, SME interview weaknesses, and system deficiencies before the agency does.
During the Inspection: Managing the Process Effectively
The Critical First Hour
How your team behaves in the first hour sets the tone for the entire inspection:
Verify credentials and Form FDA 482: Federal law requires investigators to present credentials and written notice. Review Form FDA 482 (Notice of Inspection) carefully — it specifies the inspection scope and authority.
Activate your response team via predefined notification cascade. Every team member must know their role before the call arrives.
Escort the investigator to a prepared workspace and initiate your document tracking system immediately.
Manage Document Requests Systematically
Structured document control:
- Log every request with unique identifier and timestamp
- Establish clear review hierarchy before releasing any document
- Maintain copies of all documents provided to the investigator
- Mark all copies as "Confidential" for FOIA handling
- Proactively anticipate related documents
If the investigator requests batch records for a specific product, have associated deviation reports and CAPAs ready before they ask. Fast, organized retrieval demonstrates that your quality system functions as documented — not just on paper.
Communication: Be Clear, Concise, and Factual
Train your team on these core communication rules before any investigator walks through the door:
- Clarify ambiguous questions before answering — never guess the investigator's intent
- Answer the question asked, not a broader version of it
- Never volunteer information beyond what was requested
- "I don't know, but I can find out" is acceptable; speculation is not
- When a problem is raised, focus on the investigation conducted and corrective actions taken — not on why it happened
Investigators respect companies that acknowledge issues and demonstrate systematic resolution. Defensiveness signals a weak quality culture.
War Room Operations: Stay One Step Ahead
The back room team actively anticipates the investigator's next line of inquiry:
- Hold brief morning and end-of-day meetings reviewing what was covered and preparing for tomorrow
- Keep SMEs available and on standby, even when not actively engaged
- Log all activities in writing and maintain a detailed inspection log throughout
- Use secure messaging to maintain real-time communication between front room and back room
Your war room should predict where the inspection will go next based on the documents requested and questions asked today. That forward posture — not reactive scrambling — is what separates well-prepared organizations from those that merely survive inspections.

Post-Inspection: Responding to Form FDA 483 Observations
The Critical 48 Hours
Immediate priorities after the closeout meeting:
Document all verbal and written observations while memories are fresh. Assign a scribe to capture exact wording during the closeout discussion.
Secure all inspection-related materials in one controlled location.
Schedule a debrief session immediately after the investigator departs — and again the following morning. Fatigue clouds judgment; a second debrief with fresh perspective often identifies issues missed in the immediate aftermath.
Understanding What You Received
Form FDA 483 lists inspectional observations of conditions the investigator believes may constitute violations. These are not final agency determinations — they are the investigator's observations.
A Warning Letter is different — it represents an official FDA advisory action for violations of regulatory significance, issued after center review confirms non-compliance. Warning Letters serve as formal notice before potential enforcement action.
You should respond to 483 observations within 15 business days. While no statute codifies this timeframe, FDA practice shows that timely, comprehensive responses prevent escalation.
What Makes a Strong 483 Response
Address each observation separately with clear structure:
- State whether you agree or disagree with the observation
- Describe the specific CAPA implemented or planned
- Provide realistic completion timelines
- Include supporting documentation (updated SOPs, training records, investigation reports)
- Commit senior leadership to the response — FDA wants to see executive accountability
FDA's Regulatory Procedures Manual identifies common response failures: lack of specificity, failure to address related products or sites, inadequate documentation, unrealistic timelines, no provisions for sustainability monitoring, and easily reversible "internet fixes." Vague responses that don't demonstrate prevention of recurrence are among the top reasons FDA escalates to Warning Letters.
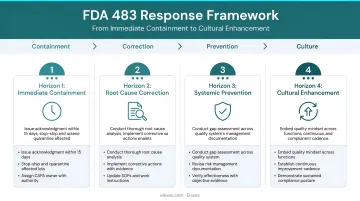
The Four-Horizon Approach to Systemic Improvement
Horizon 1 — Immediate Containment: What can be corrected right now? If the observation was missing calibration on a specific instrument, calibrate it immediately and document the calibration.
Horizon 2 — Root Cause Identification: What was the true underlying failure? Missing calibration might trace to inadequate preventive maintenance scheduling, unclear ownership of calibration responsibilities, or gaps in training.
Horizon 3 — Systemic Evaluation: Does this issue exist elsewhere in your quality system? If one instrument lacked calibration, audit your entire calibration program. Investigators respect companies that proactively expand the scope of investigation.
Horizon 4 — Cultural Enhancement: What structural changes prevent recurrence organization-wide? Perhaps you need automated calibration tracking, enhanced management review of critical equipment, or cross-functional ownership of the calibration program.
Example: Take an observation citing incomplete deviation investigations. Horizon 1 addresses gaps in individual investigation reports. Horizon 2 uncovers root causes — unclear procedures or insufficient training. Horizon 3 evaluates whether the same pattern exists across your entire deviation system. Horizon 4 examines whether your organization's culture genuinely supports quality documentation and follow-through. Companies that work through all four horizons show FDA a mature, self-correcting quality system — not just a paperwork patch.
Maintain Proactive FDA Communication
After submitting your initial response, keep momentum with consistent follow-through:
- Send monthly progress updates on significant commitments, even when FDA doesn't request them
- Document improvements with measurable outcomes — show your CAPAs delivered real change, not just updated paperwork
- Conduct a formal post-inspection review around six months out: what gaps surfaced, what's improved, and what still needs attention
Companies managing complex remediation — particularly those under multiple observations or facing QMSR transition gaps — often find it valuable to bring in specialized regulatory consulting support. An experienced partner can help structure the response strategy, track CAPA effectiveness, and run a mock re-inspection before FDA returns.
FDA Inspection Readiness Checklist for 2026
Use this structured checklist across four key domains. Frame items as yes/no questions — a "no" answer signals a gap requiring immediate attention.
Domain 1 — Documentation Systems
Document Accessibility:
- Can any trained employee retrieve a requested document within two minutes?
- Are all controlled documents within their scheduled review periods (zero overdue reviews)?
- Is there a clear audit trail documenting all changes to controlled documents?
- Does your document control system show relationships between related documents (e.g., batch records linked to applicable SOPs, deviations, and CAPAs)?
QMSR Transition Readiness:
- Have you mapped legacy DHF/DMR/DHR elements to ISO 13485 Medical Device File and record control constructs?
- Do you maintain documented evidence of FDA supplemental provisions (complaint files per 820.35, labeling controls per 820.45)?
- Are risk management activities explicitly documented across product lifecycle per ISO 13485 requirements?
Domain 2 — Personnel Readiness
Training and Competency:
- Has all staff received documented training on inspection conduct (what to say, what not to say)?
- Can SMEs explain their role, decisions, and scientific rationale without referencing documents?
- Have you conducted mock interviews with SMEs and documented their performance?
- Do you maintain role-specific competency assessments, not just training attendance records?
Response Team:
- Is your inspection readiness team identified with documented roles and backups?
- Does your rapid-response protocol specify activation procedures for unannounced inspections?
- Have you conducted at least one unannounced mock inspection in the past 12 months?
Domain 3 — Quality Systems
CAPA and Deviation Management:
- Can you demonstrate CAPA effectiveness for all past FDA observations?
- Are deviations closed within your internal target timelines?
- Do your CAPA investigations address root cause, not just immediate corrective action?
- Are post-implementation reviews documented to verify CAPA effectiveness?
Complaint Handling and Post-Market Surveillance:
- Can you show complaint trending data and medical device reporting decisions?
- Are complaint investigations complete with documented evaluation against reporting requirements?
- Does your post-market surveillance system feed into risk management file updates?
Change Control:
- Is change control documentation complete with scientific rationale for each change?
- Are post-implementation reviews documented with objective evidence of successful implementation?
- Can you trace from change requests through impact assessment, approval, implementation, and verification?
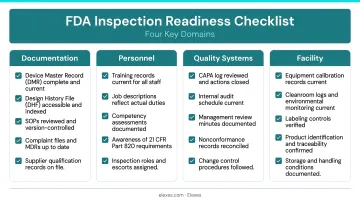
Domain 4 — Facility and Equipment
Equipment Qualification:
- Are all equipment maintenance and calibration records immediately accessible?
- Are calibration stickers current on all inspection, measuring, and test equipment?
- Do equipment logbooks document actual usage and maintenance activities?
Environmental Controls:
- Are critical utility monitoring records (temperature, humidity, air quality) current and complete?
- Are material statuses clearly identified with labels (quarantine, approved, rejected)?
- Are storage conditions documented and monitored per specifications?
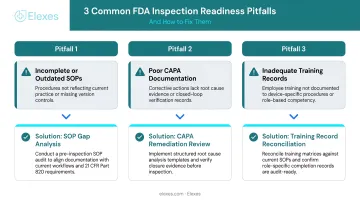
Three Common Pitfalls This Checklist Identifies
A "no" answer on any checklist item typically points to one of three root patterns. Recognizing which pattern you're dealing with determines the right corrective approach.
1. Last-Minute Preparation Syndrome
This looks like two weeks of intense activity before an expected inspection, then back to business as usual. The checklist exposes it clearly — document reviews cluster near anticipated inspection dates, and training records show activity bursts separated by months of nothing.
To address this, implement a quarterly readiness assessment cycle using this checklist. Conduct unannounced internal audits each quarter, rotate your audit focus areas, and trend findings over time. Consistency is the goal, not periodic intensity.
2. The Documentation Maze
Records scattered across paper files, shared drives, quality management systems, and email inboxes — with no clear relationships between them. When an investigator requests a batch record and the scramble begins, piecing together records from multiple systems while explaining why one reference doesn't align with another, the gap is visible immediately.
- Create a document mapping system showing relationships between all critical quality records
- Use consistent naming conventions that visually connect related documents at a glance
- Test retrieval speed monthly by randomly selecting documents and timing the process
3. The Training Gap
Staff who can recite procedures verbatim but cannot explain the underlying rationale or handle scenarios outside the script. When an investigator asks "Why do you perform this test?" and the answer is "Because the SOP says so," that response flags a training problem.
The solution is scenario-based training with documented competency assessments. Present realistic situations that require judgment, not just recall. Document demonstrated understanding through practical evaluation — not just training completion dates.
Frequently Asked Questions
What does FDA inspection readiness mean?
FDA inspection readiness is the ongoing organizational state in which documentation, quality systems, facilities, and personnel are maintained to withstand FDA scrutiny at any time. It is not a reactive preparation phase triggered by scheduled inspection notice but a continuous operational standard embedded in daily quality culture.
How do I prepare for an FDA inspection?
Effective preparation combines four elements: a cross-functional readiness team with documented backup roles, documentation retrievable within two minutes, scenario-based personnel training (not just SOP readings), and unannounced mock inspections with external auditors to surface gaps before FDA does.
How often are FDA inspections required?
The FDA uses a risk-based approach to inspection scheduling rather than a fixed calendar interval. High-risk facilities, sites with prior compliance concerns, or facilities supporting pending applications may be inspected more frequently. FDA's Site Selection Model weighs compliance history, product risk, and time since last inspection to prioritize surveillance activity.
What is a Form FDA 483?
Form FDA 483 lists inspectional observations of conditions the investigator believes may constitute regulatory violations, issued at the close of an inspection. These are not automatically confirmed violations or final agency determinations. Companies typically have 15 business days to submit a written response with corrective action plans, though this timeframe is FDA practice rather than regulatory requirement.
What are the most common FDA inspection findings for medical device companies?
FDA's fiscal year inspection observation data consistently shows inadequate CAPA investigations, incomplete or inaccurate records, failure to follow written procedures, and deficiencies in complaint handling among the most frequently cited device findings. Under the 2026 QMSR framework, inspectors are increasingly focused on design control documentation, risk management integration, and traceability between design inputs, outputs, and verification activities as they evaluate ISO 13485 alignment.
How should I respond to a Form FDA 483?
Address each observation separately with specific CAPAs, realistic timelines, supporting documentation, and senior leadership commitment. Your response must show how you will prevent recurrence — not just correct the immediate issue. FDA flags responses as inadequate when they lack specificity, ignore systemic scope, or propose easily reversible fixes — common triggers for escalation to a Warning Letter.
About Elexes
Elexes is a global regulatory affairs and quality management consulting firm supporting medical device, IVD, pharmaceutical, and biotech companies. With 50+ years of collective regulatory experience, Elexes provides FDA submission preparation, ISO 13485 implementation, QMSR transition support, mock audits, and embedded regulatory professionals. The firm has completed 250+ successful projects for 100+ global clients with a 90% audit clearance rate across FDA, MDSAP, and Notified Body inspections.