Introduction
Many medical device companies conduct internal audits on a fixed schedule, systematically working through departments year after year. Yet despite this effort, they still face repeated findings during FDA inspections and notified body assessments—often in the same process areas. The problem isn't effort; it's focus.
According to data from MD&M West 2026, the top three FDA 483 observation categories—CAPAs (12.42%), design controls (12.32%), and complaints (10.61%)—have remained virtually unchanged for approximately 17 to 20 years. This persistent pattern indicates that traditional schedule-driven audit approaches are not addressing systemic quality failures.
Risk-based internal audit (RBIA) is a direct response to that gap. This guide covers what RBIA is, how to plan and execute it under ISO 13485, FDA QMSR, MDSAP, or EU MDR, and where regulated medical device, IVD, SaMD, and biotech teams most often stumble in practice.
Key Takeaways
- RBIA prioritizes audit resources on processes and controls that carry the highest risk to patient safety, product quality, and regulatory compliance
- Unlike schedule-driven audits, RBIA is triggered and shaped by an organization's actual risk profile
- For medical device companies, RBIA maps directly to ISO 13485 §8.2.4 internal audit requirements and ISO 14971 risk management obligations
- The process runs through five stages — from scoping the risk universe to executing targeted procedures and closing findings through tracked CAPAs
- Most RBIA programs fail by treating it as a renamed compliance audit or leaving management out of the risk identification process
What Is Risk-Based Internal Audit (RBIA)?
Risk-based internal audit is a structured audit methodology that starts with the organization's risk universe rather than a departmental schedule, directing audit effort toward areas of highest potential impact on objectives, safety, and compliance.
RBIA ensures that limited audit resources deliver the greatest assurance value by concentrating on what is most likely to go wrong and cause the most harm. This approach follows methodologies defined by the Institute of Internal Auditors, which emphasizes focusing audit activity on the organization's top risks.
How RBIA Differs from Compliance Audits
Compliance audits evaluate adherence to fixed criteria — checking whether procedures exist, are signed, and follow the required format. RBIA evaluates whether the right risks are being managed well enough, regardless of whether a procedure technically exists. A process can have perfect documentation and still fail to prevent the failure it was designed to control.
Why RBIA Is Critical for Medical Device Companies
The Regulatory Mandate
ISO 13485:2016 Section 8.2.4 explicitly requires internal audits to be "planned, taking into consideration the status and importance of the processes and area to be audited, as well as the results of previous audits." This language is a direct call for risk-based planning, not uniform schedules.
The revised FDA QMSR (21 CFR Part 820) incorporates ISO 13485:2016 by reference under Section 820.10(a), making ISO 13485 Clause 8.2.4 the governing audit requirement for FDA-regulated manufacturers. The former standalone quality audit section (820.22) no longer exists.
What Goes Wrong Without RBIA
Without risk-based planning, audit resources spread evenly across low-risk administrative processes while high-risk areas like design controls, sterilization validation, supplier qualification, or software change management go under-scrutinized.
The result is repeat nonconformances during regulatory inspections. Despite conducting required internal audits for nearly two decades, the industry continues to generate the same FDA 483 observations in the same categories. As Michael Drues of Vascular Sciences noted, the industry is "practicing making mistakes."
Specific design control issues cited most frequently include:
- Not performing a risk analysis
- Not documenting the results of a risk analysis
- Failure to validate software
- Failure to confirm devices conform to defined user needs
Each of these points to a gap a well-scoped risk-based audit should catch internally—well before an FDA inspector does.
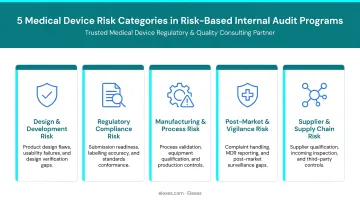
The Medical Device Risk Landscape
Identifying these failure modes is only part of the picture. RBIA must address the full risk environment medical device companies operate in:
- Design and development risks governed by ISO 14971, covering hazard identification, risk estimation, and control effectiveness
- Manufacturing process failures including sterilization validation, process controls, and production documentation
- Supply chain disruptions for critical components and supplier qualification gaps
- Post-market surveillance data gaps, with only approximately 3% to 5% of adverse events currently reported to the FDA or manufacturers
- Cybersecurity vulnerabilities in SaMD products, particularly under evolving FDA guidance
The MDSAP Angle
Companies operating under the Medical Device Single Audit Program face simultaneous scrutiny across FDA, Health Canada, TGA, ANVISA, and PMDA requirements. MDSAP now includes five RAC member authorities, eight affiliate members, and four observers, creating overlapping regulatory demands that schedule-driven audits cannot efficiently address. RBIA helps sequence and prioritize audit coverage across these frameworks.
Elexes supports medical device companies in structuring QMS audit programs around actual risk exposure under ISO 13485, MDSAP, and EU MDR. With a 90% audit clearance rate across more than 250 projects, the team helps clients prioritize high-risk processes, align audit scope to regulatory expectations, and resolve gaps before external scrutiny surfaces them.
How to Plan and Implement a Risk-Based Internal Audit
Each step in RBIA builds on the last. The structure below ensures audit resources go where the actual risk is — not where it's most convenient to look.
Step 1: Define the Audit Scope and Risk Universe
Scope definition starts by mapping your organization's processes against the applicable regulatory framework:
- Design controls (ISO 13485 Clause 7.3, 21 CFR Part 820 Subpart C)
- Production and process controls (ISO 13485 Clause 7.5, EU MDR Annex IX Section 2)
- Post-market surveillance (ISO 13485 Clause 8.2.1, EU MDR Article 83-92)
- Complaints and vigilance (ISO 13485 Clause 8.2.2, 21 CFR Part 820 Subpart M)
- Supplier management and purchasing controls (ISO 13485 Clause 7.4, MDSAP process areas)
The risk universe is a complete inventory of everything that could go wrong within these processes. This includes operational failures, regulatory compliance gaps, product quality defects, and patient safety hazards.
For SaMD products, scope must include IEC 62304 software safety classification (Class A, B, or C), which determines the rigor of development and verification processes required.
Step 2: Identify and Prioritize Risks
Risk identification draws on multiple inputs:
- Prior audit findings and CAPA history
- Complaint trends and adverse event reports
- Supplier performance data and qualification status
- Regulatory intelligence (such as recent FDA warning letters in similar device categories)
- Management interviews and process owner assessments
- Output from ISO 14971 risk management activities
Risks are then scored using a likelihood × impact matrix, typically a 1–5 scale for each dimension. High scores (above a defined threshold, such as 12 or 15 on a 25-point scale) drive audit priority.
The Institute of Internal Auditors' risk-based auditing methodology distinguishes between:
- Inherent risk: risk in the absence of any controls
- Residual risk: risk remaining after controls are applied
This distinction helps determine whether audit resources should focus on control design (are the right controls in place?) or control effectiveness (are the controls working?).
Step 3: Develop the Risk-Based Audit Plan
The audit plan allocates time, auditor expertise, and procedures proportionally to risk scores:
- High-risk areas receive more frequent and more in-depth audits
- Stable, low-risk processes may be reviewed on longer cycles or through lighter-touch monitoring
- Reserve capacity for emerging risks — a new supplier, a design change, or a regulatory update can shift priorities mid-cycle
Example allocation:
| Process Area | Risk Score | Audit Frequency | Audit Depth |
|---|---|---|---|
| Design controls | 20 (4×5) | Annually | Detailed process testing + documentation review |
| Complaint handling | 16 (4×4) | Annually | Trend analysis + root cause verification |
| Supplier qualification | 15 (3×5) | Every 18 months | Supplier audit + performance data review |
| Document control | 6 (2×3) | Every 3 years | Light-touch compliance check |

The plan should also identify which auditors are assigned to which areas based on technical expertise (such as software developers for IEC 62304 audits, or clinical specialists for post-market surveillance).
Step 4: Execute Targeted Audit Procedures
Targeted execution means developing procedures specific to each high-risk area rather than using a standard checklist. For sterilization, that means sampling batch records, verifying cycle parameters against validation protocols, and confirming deviation closure — not simply checking that a procedure document exists.
Audit evidence should be evaluated against risk appetite, not just binary pass/fail criteria. If a process shows minor documentation gaps but strong control effectiveness, the audit finding should reflect that nuance.
Auditors should also assess whether the organization is monitoring the effectiveness of risk controls, as required by ISO 14971. This means checking not just that controls exist, but that the organization has data demonstrating they are working.
Step 5: Report Findings and Track Corrective Actions
RBIA outputs should directly link findings to the risk universe, making it clear to leadership which risks remain elevated and why. Reports should include:
- Process area audited
- Risk score that triggered the audit
- Findings (nonconformances, observations, opportunities for improvement)
- Root cause analysis (where applicable)
- Assigned CAPA owners and timelines
- Expected impact on residual risk after CAPA closure
CAPAs must be tracked to verified closure. Verification should confirm that the corrective action addressed the root cause — not just that a response was documented — and that the associated risk score has been reassessed accordingly.
Key Factors That Affect RBIA Effectiveness in Medical Device Environments
Data Quality and Availability
The reliability of RBIA depends heavily on the inputs used to build the risk universe. Companies with incomplete CAPA records, underdocumented complaint trends, or no formal supplier risk scoring will produce inaccurate risk prioritization.
How to strengthen these inputs before beginning RBIA planning:
- Categorize all CAPAs by process area and root cause through a retrospective review; identify recurring themes
- Implement structured complaint coding (by device, failure mode, severity) and run quarterly trend analysis
- Build a supplier risk matrix based on component criticality, performance history, and regulatory compliance status
- Subscribe to FDA 483 observation databases, warning letter trackers, and MDSAP audit reports for regulatory intelligence
Without these inputs, risk scoring becomes subjective and audit plans become guesswork.
Regulatory and Product Complexity
Device classification, intended use, and applicable regulations directly determine which processes receive audit priority.
Examples of how complexity drives audit focus:
| Device Type | Risk Focus | Audit Priority Areas |
|---|---|---|
| Class III implantable | Biocompatibility, sterility, design validation | Sterilization validation, design controls, supplier qualification |
| SaMD Class C (IEC 62304) | Software defects causing serious injury or death | Software verification/validation, cybersecurity controls, change management |
| IVD (EU IVDR) | Analytical/clinical performance, intended use claims | Clinical evidence, post-market performance monitoring, labeling accuracy |
| Class I exempt | General controls only | Minimal audit depth; focus on labeling and reporting |
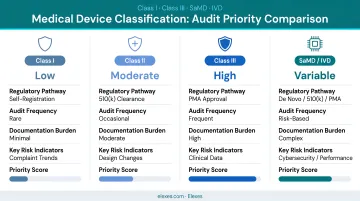
A Class I device manufacturer conducting the same audit depth as a Class III implant manufacturer is wasting resources. On the flip side, a SaMD developer auditing document control annually while auditing software change management every three years is inviting regulatory findings.
Organizational Factors
Two organizational factors determine RBIA quality more than any other: management involvement and audit team independence.
Senior leadership must participate in risk prioritization and sign off on the audit plan. This ensures audit resources align with strategic priorities and that findings receive executive attention. Without that buy-in, RBIA becomes a compliance exercise that nobody acts on.
Auditor independence is equally non-negotiable. ISO 13485 Clause 8.2.4 is explicit: "Auditors shall not audit their own work." Organizations that allow process owners to audit their own areas undermine audit credibility and expose themselves to regulatory defensibility challenges during inspections.
Common Issues and Misconceptions in RBIA
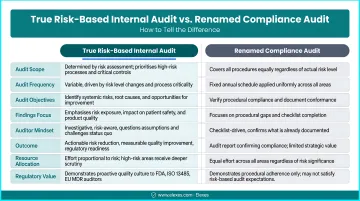
Misconception: RBIA Is Just a Relabeled Compliance Audit
The most common misconception is that RBIA is simply a compliance audit with a new name. In practice, many organizations rename their existing schedule-based audit program "risk-based" without actually adjusting priorities based on risk scores.
RBIA changes what gets audited and how deeply — not just what it is called. A true RBIA program:
- Audits high-risk areas more frequently than low-risk areas
- Uses risk scores to determine audit depth and procedures
- Adjusts the audit plan when new risks emerge
- Links findings back to the risk universe in audit reports
A renamed compliance audit:
- Audits all areas on the same fixed schedule
- Uses the same checklist for every audit
- Does not adjust priorities based on risk
- Reports findings without reference to risk scores
Overemphasis on Documentation Review vs. Process Effectiveness Testing
Teams frequently overemphasize documentation review — checking if SOPs exist and are signed — at the expense of testing whether the process actually prevents the failure it was designed to prevent.
Regulators identify this gap during inspections as the difference between an audit that found nothing and a process that is actively failing. The 17-20 year persistence of identical FDA 483 observation categories is the clearest evidence that documentation-focused audits have not driven systemic improvement.
Process effectiveness testing looks like:
- Sampling batch records to verify sterilization parameters match validation protocols
- Testing whether complaint trending analysis is actually used to trigger CAPAs
- Verifying that supplier qualification criteria are applied consistently across all new suppliers
- Checking whether post-market surveillance data is reviewed and acted upon
When RBIA May Not Be the Right Fit
RBIA isn't the right fit for every organization. For very small teams with a narrow product scope and stable processes, a full risk-universe-driven approach can create overhead that outweighs the benefit.
A simpler, focused compliance audit may be more appropriate when:
- Startup with a single Class I device and fewer than 10 employees
- Stable process environment with no significant changes, complaints, or CAPAs in the past 2 years
- Limited resources with no dedicated quality or regulatory staff
That said, ISO 13485 still requires some consideration of risk in audit planning — even at small scale. A startup might use a simple high/medium/low risk assessment rather than a full risk matrix, but the principle of directing audit effort toward higher-risk areas still applies.
Frequently Asked Questions
What is a risk-based internal audit?
RBIA is an audit methodology that directs audit focus and resources toward the processes and areas carrying the highest risk to the organization's objectives, safety, or compliance, rather than following a fixed departmental rotation. It uses risk scoring to prioritize audit effort.
What are the main types of risk in internal audit?
RBIA typically assesses five core risk categories:
- Operational: manufacturing failures, process breakdowns
- Regulatory/compliance: FDA 483 observations, audit nonconformances
- Product quality and safety: device defects, labeling errors
- Strategic: supplier dependencies, outsourced functions
- Medical device-specific: design integrity, software (IEC 62304), supply chain
How do you prepare a risk-based internal audit plan?
Start by building a risk universe from process maps and regulatory requirements. Score each area by likelihood and impact, prioritize high-scoring processes for greater audit depth and frequency, and document your rationale. The final plan should cover objectives, scope, methods, schedule, and reporting protocols.
What is included in an internal audit plan?
A complete audit plan covers objectives and scope, the processes to be audited, the methods and criteria used, the schedule and resource allocation, and reporting and follow-up protocols. Auditor assignments and independence controls should also be documented.
How often should a risk-based audit be performed?
ISO 13485 requires audits at planned intervals but does not set a fixed frequency. In RBIA, high-risk areas are typically audited more frequently (such as annually or after significant changes) while stable, low-risk processes may be reviewed on longer cycles (every 2–3 years, for example).
What are the stages of the internal audit process?
The standard stages include planning and scope definition, risk identification and prioritization, audit execution and evidence collection, findings documentation and reporting, and corrective action follow-up and closure verification. Each stage feeds into the next to create a continuous improvement cycle.